Supporting New Ireland Province to Advance Lymphatic Filariasis (LF) Elimination: Preparation and Training for the Second Transmission Assessment Survey
In October 2025, New Ireland Province (NIP) undertook its second Transmission Assessment Survey (TAS) to assess whether transmission of Lymphatic Filariasis (LF) has remained at levels low enough to progress toward elimination. The survey was carried out in line with World Health Organization (WHO) recommended procedures, and the results will undergo formal review by WHO. This update provides an overview of the preparatory work and pre-survey training conducted ahead of the second TAS, as well as the province’s long-standing efforts to combat LF.
Background: Progress to Date in New Ireland Province
New Ireland Province has long served as one of Papua New Guinea’s (PNG) leading provinces in advancing efforts to eliminate LF
.
In 2011, the National Department of Health (NDoH) conducted a baseline survey*1, which confirmed an antigen prevalence of 15–17% using the Immuno-Chromatographic Test (ICT). This placed the province in the hyperendemic category, underscoring the need for urgent intervention. Following this finding,
the first Mass Drug Administration (MDA) using a two-drug regimen, Diethylcarbamazine (DEC) and Albendazole
, was implemented in 2014 with support from external development partners, achieving 78% treatment coverage
. WHO supported the subsequent second and third rounds of MDA in 2015 and 2016, achieving strong results with 87% and 78% coverage respectively.
In November 2017,
WHO recommended the introduction of a new triple-drug therapy, Ivermectin, DEC and Albendazole (IDA)*2
, after international clinical trials demonstrated its superior effect on adult worms and its potential to shorten the number of MDA rounds required to interrupt transmission.
Responding to this global shift, JICA joined the PNG national effort through a technical cooperation project, supporting the implementation of
the fourth round of MDA using IDA in December 2018
. Despite significant challenges including a nationwide polio outbreak, overlapping polio vaccination campaigns and the Christmas holiday period, as a result, the campaign reached 67.1% coverage.
Transition to Post-MDA Surveillance and the Need for the second TAS
Following MDA completion, NIP entered the post-MDA surveillance stage.
The first TAS
was planned for 2020 but was delayed due to COVID-19. It was eventually
carried out between December 2020 and March 2021
, with additional targeted surveys undertaken in August 2021 in locations where suspected positives were detected.
The final results showed an extremely low antigen prevalence of 0.17%, leading WHO to issue a “Pass” determination
, indicating no further MDA was required at this time.
Under the standard elimination pathway, three rounds of TAS are to be conducted at two-year intervals. However, progress towards the second TAS had stalled due to ongoing coordination challenges with other priority activities. The implementation of the second TAS in 2025, therefore, represents a major step in resuming the elimination pathway and validating the province’s sustained suppression of LF transmission.
Progress to Date in New Ireland Province
| Year | Activities | JICA Project |
|---|---|---|
| 2011 | A baseline survey for LF was conducted. ICT results showed an antigen prevalence of 15–17%, confirming the province as hyperendemic. | Grant Aid: Provision of Special Medical Equipment for Infection Control Phase 1-4 — provided DEC tablets, ICT kits, and LF diagnostic kits across 14 Pacific countries (PNG received LF test kits in 2016 only). |
| 2014 | The first round of MDA using the two-drug regimen DEC + Albendazole) was implemented, achieving 78% coverage. Key support: USAID, FHI360, WHO |
|
| 2015 | The second round of MDA (two-drug regimen) was implemented, achieving 87% coverage. Key support: WHO |
|
| 2016 | The third round of MDA (two-drug regimen) was implemented, achieving 78% coverage. Key support: WHO |
|
| 2017 | A mid-term survey confirmed an antigen prevalence of 0.3%, indicating very low infection levels. In November, WHO recommended the introduction of IDA triple-drug therapy (Ivermectin + DEC + Albendazole). |
|
| 2018 | The fourth round of MDA, and the first using IDA therapy, was implemented, achieving 67.1% coverage.
Key support: WHO, JICA |
Technical Cooperation: Project for Elimination of Lymphatic Filariasis in the Pacific Region -Phase 1 (Oct 2018–Feb 2022; extended one year due to COVID-19, completed Feb 2023). |
| 2020 |
The first TAS was conducted from December 2020 to March 2021. Key support: WHO, JICA, PNG Institute of Medical Research |
|
| 2021 | In August, an additional survey was carried out in areas where suspected positives were detected in the first TAS. The first TAS result: 0.17% antigen prevalence, WHO assessment: “Pass” (no further MDA required). |
Challenges in Determining the Target Population
In PNG, reliable demographic data generally remains difficult to obtain, not only in the health sector but across many areas of government planning. The most recent national census prior to this survey was conducted in 2011, and although a new census took place in 2024, results had not been fully released as of July 2025. Therefore,
the province has been unable to obtain updated population statistics for the target group of 6–7-year-old children (Grade 1 and Grade 2)*3, and preparations for conducting the second TAS have consequently been unable to progress
.
To address this issue, our project team travelled to Kavieng in August 2025 with colleagues from the NDoH and WHO to review the situation with relevant authorities. The team confirmed that the Provincial Education Office also lacked accurate and current enrolment figures. Based on this situation, the sampling methodology was revised,
shifting from the School-Based approach to the Community-Based survey using Local-Level Governments (LLGs) as the sampling unit
. Using preliminary 2024 census data available to the New Ireland Provincial Health Authority (PHA), WHO identified survey clusters*4 and population targets in accordance with its global guidelines.
Following the confirmation of target populations, the survey micro-plan and budget were finalised. Cost-sharing arrangements between WHO, PHA and the JICA project team were agreed. The JICA project committed to supporting procurement and transport of survey items, preparation and delivery of training for health workers, coverage of some operational costs during implementation, and data management.
Establishing cost-sharing arrangements is essential for securing strong ownership and commitment among implementing partners
.
Location of New Ireland Province (highlighted in red) – map created using MapChart.

Discussion with PHA officials and the visiting team regarding target population estimates (Kavieng, August 2025).
Pre-Survey Training for Field Teams
On 21 October 2025,
the training for PHA health workers was conducted in Kavieng in preparation for the second TAS
. A total of 34 participants attended, including field surveyors and supervisory staff. Sessions covered an overview of LF, survey methodology, logistics and reporting requirements, alongside practical exercises in blood sampling and survey itinerary planning. Lectures were delivered by officers from the NDoH, WHO, and the JICA project team.
For this TAS, a new diagnostic tool,
the STANDARD Q Filariasis Antigen Test (QFAT), procured by WHO, was introduced for the first time in PNG
.
QFAT has demonstrated higher sensitivity in recent international field evaluations
compared with the previously used Filariasis Test Strip (FTS), and is increasingly regarded as a reliable, user-friendly rapid diagnostic tool. During practical sessions, participants worked in pairs or small groups to practise finger-prick blood collection and test procedures. Many attendees had prior experience with the first TAS or routine blood collection, contributing to smooth training delivery. The training was highly practical, and participants demonstrated strong understanding of survey objectives and key considerations.

WHO Technical officer explaining the survey protocol.

JICA expert providing guidance on logistics and reporting procedures.

Health workers practising blood collection using the QFAT kit.
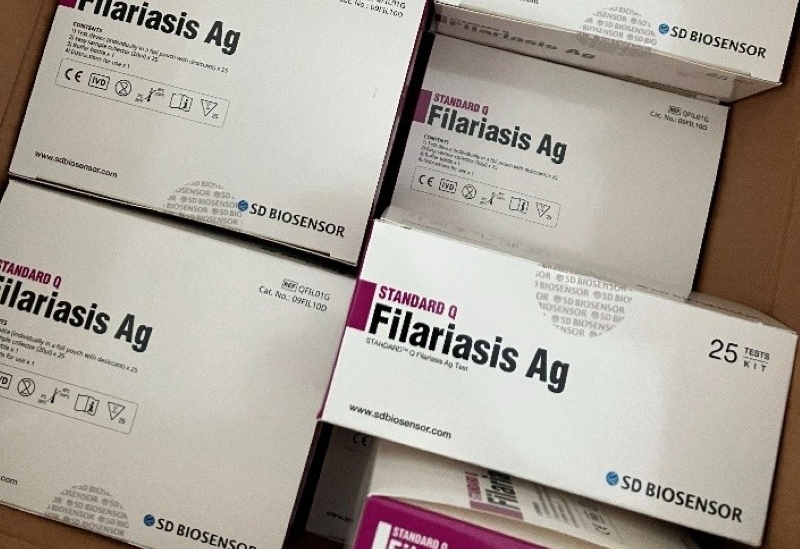
QFAT-LF diagnostic kit supplied through WHO procurement.

Team discussions on survey planning – Namatanai District.

Team discussions on survey planning – Kavieng District.
Prior to the training, the JICA project team checked the survey materials dispatched from Port Moresby and worked with medical store-warehouse staff to sort items into team bags . More than 20 types of supplies, including safety lancet and swabs, IEC awareness material and stationaries, were prepared and packed for 14 field teams.

NIPHA staff sorting survey materials at the medical warehouse.

Survey materials prepared into 28 bags (two per team for a total of 14 teams).
The second TAS represents an important milestone in NIP’s progress towards verification of LF elimination
. The survey is led by the PHA, with oversight from the NDoH and WHO, and other technical and logistical support from the JICA project.
TAS is an essential activity for detecting any residual risk of LF transmission and for assessing the epidemiological situation following the cessation of MDA
. Fourteen survey teams are conducting implementation over a two-week period, after which data will be compiled and analysed.
Furthermore,
teams were instructed to complete a line-listing form and report any individuals suspected of having LF-related lymphoedema or hydrocele
during the course of the survey. Although the PNG Government acknowledges that LF cases persist, available case information remains limited,
making it essential to continuously update the understanding of the current patient situation
. LF can cause severe damage to the lymphatic system, leading to conditions such as lymphoedema and elephantiasis, in which limbs become significantly hard and swollen.
These chronic disabilities not only hinder a person’s ability to work and contribute to poverty, but also lead to social stigma due to visible changes in appearance. As a result, many patients avoid going out or experience mobility difficulties, which further reduces their access to health services
. Together, these factors make it even more challenging to accurately identify and monitor LF cases in affected communities.
Survey results will be submitted to WHO for independent evaluation, which will determine the province’s next steps in the LF elimination pathway.
Survey Overview
| 1. Survey Title / Objective |
The second Transmission Assessment Survey (TAS) – Second-round LF transmission assessment To evaluate ongoing transmission of LF following completion of MDA and determine whether further MDA is required. |
| 2. Target Population | A total of 1,560 children aged 6–7 years (Primary Grades 1–2). (As per WHO guidelines: 52 children per cluster selected from 30 wards across the province, based on parental consent. Sampling is drawn from schools or LLG-based communities, totalling 1,560 eligible children) |
| 3. Survey Period | October–November 2025 (approx. two weeks of field implementation). |
| 4. Survey Methodology | - Rapid antigen testing using STANDARD Q Filariasis Antigen Test (QFAT) to confirm Positive or Negative cases; IDA treatment provided for positive cases. - LLG-based sampling approach. - EA (Enumeration Areas) selection using the WHO Survey Sample Builder (SSB) in line with WHO guidelines. - Line-listing report of any individuals suspected of having LF. |
| 5. Survey Implementation Structure | - Fieldwork carried out by 14 PHA survey teams, each consisting of at least five members (1 team leader/health worker, 1 trained assistant health worker, 2 community volunteers, and local 1 driver or operations assistant). - Oversight and technical support from the NDoH and WHO - Financial and logistical support shared among PHA, WHO and JICA Project. - Survey conducted following pre-survey training for all health workers. |
| 6. Use of Results | Survey results will be submitted to WHO for evaluation and will inform future LF elimination strategies, including the need for any additional MDA. |
Footnotes
*1 Baseline surveys are conducted before the introduction of MDA to determine LF infection prevalence, antigen positivity rates, geographic distribution and associated risk factors within the target area.
*2 WHO recommended the introduction of IDA therapy based on multiple international clinical studies demonstrating that IDA has superior parasite-clearing effects compared with the traditional two-drug regimen, including inactivation of adult worm nests. This enables faster interruption of transmission and can significantly reduce the number of MDA rounds required. (Ref.:
WHO Guideline – Alternative mass drug administration regimens to eliminate lymphatic filariasis, 2017.)
*3 WHO identifies children aged 6–7 years as the optimal target group for TAS because:1. They best reflect recent transmission, 2. Positive cases are more likely to be detected if transmission is ongoing, and 3. Surveys are operationally efficient among this age group. (Ref.: Lymphatic filariasis: monitoring and epidemiological assessment of mass drug administration – A manual for national elimination programmes, WHO, 2011.)
*4 Sampling areas were determined using the WHO Survey Sample Builder (SSB), an online tool that automatically calculates sample size and selects survey clusters (Enumeration Areas) for TAS based on WHO methodology.
For more information:
Preparing for the Second Lymphatic Filariasis Transmission Survey in New Ireland Province (12 November 2025, JICA PNG Office)
- Media coverage
New Ireland steps up Filariasis fight as partners back transmission survey (03 November 2025, National Broadcasting Corporation (NBC) Online)
- Reference
Papua New Guinea steps up efforts to eliminate lymphatic filariasis (28 September 2021, WHO Global News)