[Update]Achievements observed in Lymphatic Filariasis (LF) Mass Drug Administration (MDA) activities in West New Britain Province
The principal counterpart organisations for this project are the Papua New Guinea (PNG) National Department of Health (NDoH) and the respective Provincial Health Authorities (PHAs). As the PHAs oversee the health facilities responsible for delivering Mass Drug Administration (MDA), the success of activities has depended on close coordination with them, as well as with representatives from each health facility.
MDA is provided to almost the entire population of the province. However, not all towns and villages have reliable road infrastructure, and some communities – including outer islands – can only be reached by small boats via sea routes. For this reason, strong leadership and initiative from the PHAs, who best understand local geography and security conditions, are essential for the effective delivery of MDA.
In this round, the West New Britain Provincial Health Authority (WNBPHA) demonstrated strong leadership, enabling the successful completion of MDA activities. Moreover, several outcomes were achieved that will contribute to strengthening organisational capacity into the future. The following activities during MDAs are good examples of these achievements.
Strong Commitment from Counterpart Agencies
Strengthened Organisational Leadership
Based on lessons learned from the first round of MDA, it was recognised that strengthening the operational structure was essential for the successful delivery of the second round. To this end,
in order to implement an effective MDA, WNBPHA utilised the existing organisational structure of the Provincial Emergency Operations Centre (PEOC) as the Technical Working Group (TWG) for the MDA.
The PEOC was led by the Director of Public Health (DPH) and structured into functional teams responsible for operations, communications and public awareness, partner coordination, planning and monitoring, medical logistics and warehouse, and finance. Representatives from the PHA were assigned to each team. In addition, local-level government (LLG) representatives, church groups, media personnel, and private sector stakeholders from communities across the province participated, with clearly defined roles to ensure smooth implementation of activities.
Regular PEOC meetings were held to discuss progress and address challenges promptly, while ensuring fair and efficient information sharing. Given that some of the 37 health facilities in the province are managed by church organisations or palm oil companies, collaboration with these institutions was also essential. A WhatsApp group was created as a communication channel among PEOC members. While its original role concluded after the MDA, the group is planned to be maintained and utilised for other programmes, contributing to a sustained and effective communication system within the PHA.

PEOC regular meeting

Group photo after pre-MDA training at Silanga Health Centre, one of the church-managed health facilities
Access to People Living in Remote Areas
In PNG, social infrastructure such as roads and bridges is not sufficiently developed, and many hard-to-reach areas (HTRA) exist across the country . In many health facilities, there is a chronic shortage of healthcare workers to address various health issues. In these areas, it is challenging to provide stable public health services or ensure that residents can visit health facilities, making it difficult to say that the health service delivery system is fully established. Furthermore, due to changes in employment opportunities and environmental factors, population movements are observed, making it difficult to accurately capture the latest demographic data. Against this backdrop, visiting individual villages through large-scale public health activities such as Mass Drug Administration (MDA) is considered highly effective not only for providing health service opportunities but also for gathering up-to-date information on population size, living conditions, and the local environment .

MDA team walking through bushland to reach villages (Eseli Health Centre)

MDA team travelling by road tractor in Unea, where no proper roads have been developed on the island (Unea Health Centre).
To reach HTRAs where medical access is extremely limited, WNBPHA arranged private helicopters to transport drug administration teams and carry out the MDA activities. In these hard-to-reach areas, some teams made the most of their visits by not only conducting MDA but also providing additional medical support, such as malaria testing and treatment for other diseases, ensuring that all residents could receive as much health service as possible during the visit.

MDA team loading items onto a helicopter to reach an HTRA (Kaliai Health Centre)

Aerial view of the catchment area from a helicopter (Buvussi Health Centre)
Human Resource Allocation
Number of MDA Field Workers
MDA activities require the mobilisation of large numbers of personnel to carry out intensive MDA within a limited period. In the second round of MDA,
246 health workers were engaged in field operations, supported by an additional 370 community volunteers who assisted with logistics and liaising with local communities.
Prior to implementation, representatives from health facilities who had received training in Kimbe, conducted pre-MDA training sessions in their respective areas. All field members were provided with daily allowances through the PHA, based on the number of days they participated in MDA activities.
Each health facility was tasked with maintaining routine medical services while planning efficiently to dedicate limited staff to MDA operations. Undertaking public health campaigns on such a large scale is rare, and the quality of preparation and planning directly influenced outcomes.
Unity and cooperation within communities were also essential to success
. Nonetheless, unpredictable factors such as weather and security challenges often arose, requiring flexible responses on the ground.

Pre-MDA training session (Melenglo Health Centre)

Hard works from community leaders and local volunteers, who have a strong understanding of the communities, was indispensable (Wako Health Centre)
Measures to Improve MDA Coverage Rates
The size and geographical conditions of the catchment areas for each health facility varied greatly. In particular, one community health facility located in the provincial capital, Kimbe, faced challenges during the first MDA because its catchment population was extremely large, the residential areas were widely dispersed, and some villages had poor road access, resulting in stagnant drug coverage rates. In response to this situation, for the second round of MDA, the staffing structure was strengthened from the budget planning stage by adding a team from Kimbe Provincial Hospital to help cover the area. As a result, the community health facility in Kimbe and the provincial hospital worked together to complete drug administration for more than 30,000 residents across 141 sites in 32 villages within the Kimbe catchment area. This strategic allocation of personnel contributed significantly to improving the drug coverage rate.

Health worker writing the alphabet corresponding to the correct dosage on a participant’s hand, determined by measuring height (Kimbe Health Centre, KUC)

MDA team explaining the activity to lower-grade students at a school (Kimbe Provincial Hospital Team)
Financial Commitment and Resource Mobilisation
Securing Grants from the Provincial Government
The primary budget required for MDA implementation was largely covered through external donor support channelled via the World Health Organization (WHO).
At present, financial contributions from the PNG Government remain very limited, which poses a major challenge to sustaining this initiative.
Each round of MDA in the province costs more than JPY 100 million (approximately USD 680K)
, making continued implementation impossible without external funding.
During the budget planning for the second round of MDA, a team from NDoH delivered a presentation to the Governor of WNBP, requesting support. Despite the province facing significant financial constraints,
the Governor Sasindran Muthuvel recognised the importance of the activity and approved a grant of PGK 500,000 (approx. JPY 18 million, around USD 122K).
This funding, processed through the PHA, was allocated for activities such as organising the MDA launch ceremony, helicopter hire, procurement of Azithromycin (for yaws treatment), coverage assessment surveys, radio publicity, and other operational expenses. This contribution played a critical role in the smooth execution and enhanced effectiveness of the MDA. The PHA, despite having only a small finance team, the Health Services Improvement Program (HSIP), successfully handled a large volume of transactions accurately and as promptly as possible, contributing greatly to the MDA. In addition, the PHA demonstrated its financial commitment by covering travel and vehicle expenses for transporting medicines and supplies to health facilities across the province.

Handing over of the cheque board from the WNBP Governor Sasindran Muthuvel to the WNBPHA CEO

Presentation by PHA finance staff on accounting procedures during pre-MDA training for health facility representatives
Collaboration and Support from Other Health Programs
Given the recognised challenges of securing sufficient funding, the PHA sought to coordinate with other health programs during MDA implementation, aiming for more efficient use of resources and cost savings. For instance, training schedules were aligned with those of other programs so that staff from remote health facilities travelling to Kimbe by dinghy boats could combine activities. This reduced transport and fuel costs by integrating MDA-related training with other program activities. Through this approach, support was secured from Australian Doctors International (ADI) *1, the provincial branch of an Australian NGO. ADI not only covered transport and fuel expenses but also provided financial support for the MDA launch ceremony. Beyond this, contributions and in-kind support were also received from schools, church groups, local police, logging companies, palm oil producers, and community members, creating a collaborative framework in which the whole community worked together to drive the campaign forward.

Health facility representatives arriving at the boat landing site in Gloucester for their return journey.

Transport of medicines and supplies to health facilities often required carrying fuel drums along with the items for delivery.
Strengthening Public Awareness for the MDA Campaign
During the second round of MDA, public awareness activities were significantly strengthened, led mainly by PHA stakeholders. The following initiatives were implemented:
Launch Ceremony for MDA Implementation
A launch ceremony was held in Kimbe town to officially announce the commencement of the MDA. Representatives from the PHA, NDoH, and the JICA expert took the stage to highlight the objectives and significance of the campaign. To demonstrate the safety of the medicine, officials also took the tablets themselves in front of the audience. At the same time, local health facilities set up treatment booths at the venue, allowing residents who wished to participate to receive the medication. On the following day, Governor Sasindran Muthuvel also publicly took the medicine at the PHA venue, reaffirming the provincial government’s commitment to the MDA. Videos of these events were shared among stakeholders via WhatsApp, and health facility staff later reported that they had been able to use the footage as a practical tool to explain the safety of the drugs to surrounding communities and residents in remote villages.

PHA Director of Public Health calling on residents to take the medication

Stage set up for the launch ceremony in Kimbe town.
Clear Messages to Residents through Megaphone Speakers
To improve community outreach, megaphone speakers were distributed to each MDA team. During the first round of MDA, community feedback indicated confusion, with some residents reporting that they either did not understand the campaign or were unaware it was taking place. A key reason was that the voices of health workers during mobilisation did not effectively reach residents. To address this, the LF national team developed a script of standardised health messages, which was distributed together with megaphones for the second round. This enabled teams to deliver clear and consistent messages in a timely way, both to residents inside their homes and to those working outdoors. While some teams had independently used megaphones or sound equipment in the first round, usage and methods varied. By introducing a unified approach this time, communication was strengthened, contributing to improved treatment coverage. Procuring a sufficient number of megaphones in PNG proved challenging, as very few suppliers held stock. Considerable time and effort were required to source 140 units, which were eventually provided to the PHA.

Procured megaphones, later labelled with the JICA logo and Japanese national flags

Community awareness on MDA using the distributed megaphones in Bialla town, Nakanai District (Bialla Health Centre)
Collaboration with Local Radio Station
Since representatives from the National Broadcasting Corporation (NBC) Kimbe branch – the state-owned radio station – were members of the PEOC, radio promotions for the MDA, including commercial jingles and Talk Back Show programs, were smoothly coordinated. In the first round, communication activities had been managed mainly by this project team, but by the second round the PEOC had taken the lead in planning and implementing these efforts, resulting in stronger public outreach.

NDoH and PHA communication officers providing an overview of the MDA on a Talk Back Show

The NBC radio station building in Kimbe
Sharing MDA Updates on Social Media
The PEOC communication team also launched a dedicated Facebook account to actively share updates on the progress of the MDA and related information.
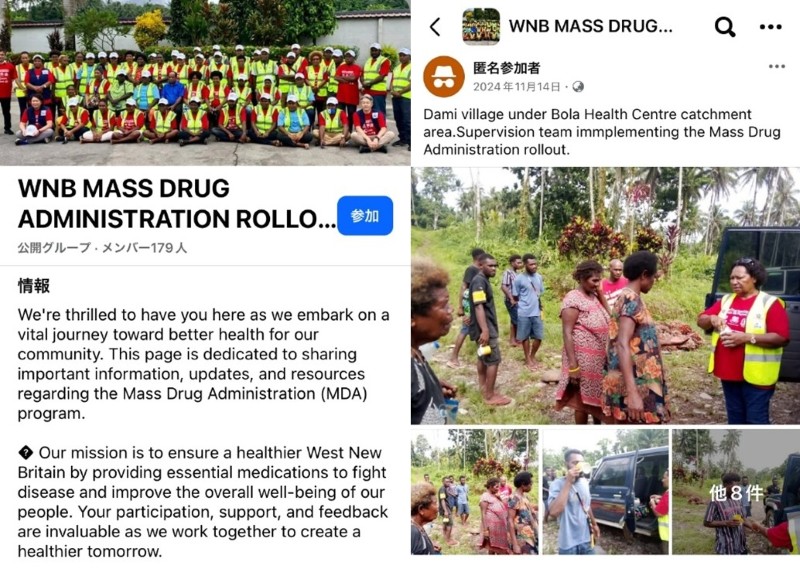
WNBP MDA activities were publicised through a dedicated Facebook account.
Efficient Field Operations with Limited Budgets and Resources
Coordination with Field Staff
Streamlining Sorting and Delivery of MDA items
In addition to medicines, a range of other supplies was needed to keep the MDA running smoothly. These included campaign T-shirts, caps and safety vests for staff; posters and banners for raising awareness; and various recording forms and stationery. Altogether, more than 20 different items had to be managed alongside the medicines. As some materials from the first round could be reused, the total number of items required in the second round was slightly reduced.
Distributing these supplies to each health facility was more than just a logistical exercise – it formed a vital foundation for the community drug administration
. Getting the right items to the right place on time helped avoid confusion on the ground and ensured the MDA could be carried out as planned. Because the volume of supplies varied with the size of each health facility, the project prepared a detailed distribution list. Items were carefully sorted and packed into outer bags clearly labelled with the name of each facility. The sorting took several days, with PHA medical warehouse staff working side by side with the project team. Carried out in a warehouse without air conditioning, the work was physically tough, and we remain deeply grateful to everyone who worked tirelessly under such demanding conditions.
For the second round, a few extra adjustments were introduced to make operations run more smoothly. Reporting forms were simplified and combined, while campaign T-shirts were standardised with only limited colours and sizes. This helped ease the workload of inventory management and sorting. All of these changes were carefully planned to ensure there was no disruption to field operations.

Sorting operations carried out intensively over a short period by a 5–6 person team

For larger health facilities, more than 10 small boxes and bags were prepared, temporarily filling the medical warehouse with MDA items
Exploring Efficient Delivery Methods
In the first round of MDA, medicines and items were mainly distributed by having representatives from each health facility carry them back after attending the pre-MDA training in Kimbe. While this seemed practical at first, it also carried potential risks of theft, loss, or damage along the way. By the second round, lessons had been learned. To make the process safer and more efficient,
this project chartered trucks and transport ships, with PHA staff accompanying the deliveries to ensure everything reached the right places on time.
Plans had initially called for using PHA-owned trucks, but when one broke down, the team had to adapt quickly and make alternative arrangements.
Delivery methods were tailored to the geography and circumstances of each facility:
・Nearby health facilities: collected their own items directly from the warehouse.
・Facilities accessible by road: received consolidated deliveries by truck.
・Island facilities: items were delivered alongside training sessions or monitoring visits.
・Remote coastal facilities: chartered mid-sized ships delivered the items within a few days.
By choosing the right method for each location, the team managed to distribute items both safely and efficiently.

PHA staff cross-checking delivery quantities against distribution lists at Pililo Health Centre

Item bags being carefully loaded one by one onto a chartered ship at the Kimbe wharf
Improving Collection of Treatment Record Forms
In PNG, many rural areas still lack a reliable communication infrastructure, so asking health facilities to submit data online simply isn’t realistic. The most practical solution was still to use paper treatment record forms, collected and processed later at central hubs. However, in the first round, delays in collecting these forms created bottlenecks in compiling the data. Determined not to repeat the same problem, the team introduced a new approach for the second round:
- Data entry teams based in the provincial capital travelled out to health facilities accessible by road and collected the forms directly. This allowed health workers to focus on their own tasks while the data teams pushed ahead with timely processing.
- Because the teams were made up of experienced staff from the first round, they were already familiar with the process, which made the work run more smoothly.
The project supported these teams by covering operating costs, including vehicle hires for form collection. At the same time, a lighter but very effective addition was introduced: each health facility was asked to send a photo of its summary sheet via WhatsApp. This gave the team an early snapshot of results, even before the paper forms arrived.

Staff carrying out data entry management at PHA headquarters in Kimbe
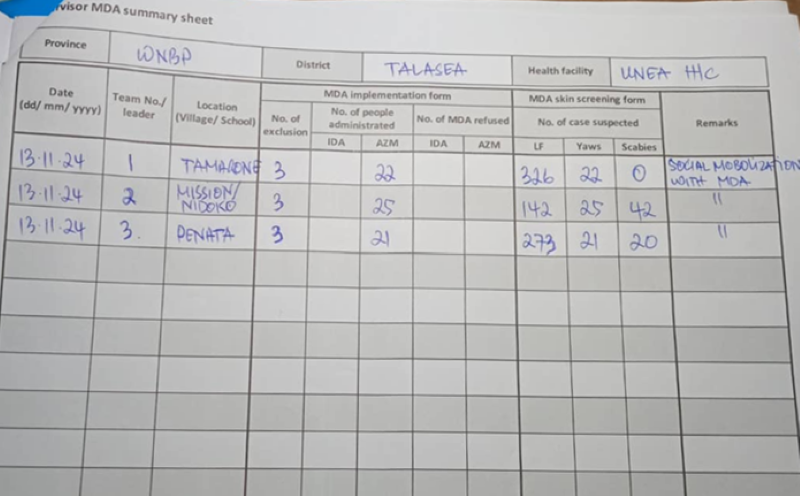
A quick snapshot of summary data sent via WhatsApp (Unea Health Centre)
Looking back, these experiences highlight an important point. PNG is steadily decentralising responsibilities between the national and provincial governments, and even within provinces, the way health services are organised can differ. That means public health activities must be flexible, designed to fit the realities of each place. And above all, keeping open lines of communication—with institutions, communities, and frontline staff—remains the key to making support truly effective.
*1 An Australian non-profit NGO, primarily focused on rural and island areas of PNG, providing medical support and working to strengthen the capacity of local personnel.
For more information, visit the JICA PNG Office website;
- Official Launch of Mass Drug Administration (MDA) Round 2 in West New Britain Province; The Project for Elimination of Lymphatic Filariasis Phase 2 (2024.12.09)
- Working Together for a Lymphatic Filariasis-Free Future: Post-MDA Workshop (2025.05.28)