[Update] Lymphatic Filariasis Response in East New Britain Province: Focal MDA Following IDA Impact Survey
In East New Britain Province (ENBP), the first IDA Impact Survey (IIS) following the Mass Drug Administration (MDA) for lymphatic filariasis (LF), conducted in June 2024, was completed. The survey identified areas where there was a potential risk of continued LF transmission. In response, a localised additional MDA (focal MDA) was implemented targeting these areas. The focal MDA was carried out across four locations in ENBP, reaching approximately 2,300 people and achieving a high overall coverage rate of 95.2%. No serious adverse events or incidents were reported, and the activities were completed safely. This intervention focused on areas with a higher risk of transmission and is expected to contribute to reducing residual transmission.
Background and MDA History
ENBP has been implementing sustained efforts towards LF elimination over the past several years. Since 2019, the province has adopted the WHO-recommended triple-drug regimen (ivermectin, diethylcarbamazine (DEC), and albendazole—IDA). The first round of MDA, conducted in 2019, achieved a coverage rate of 82.2%, significantly exceeding the WHO-recommended threshold of 65%, with approximately 300,000 people treated out of a total provincial population of around 370,000. Although the second round was initially scheduled for 2020, it was delayed due to the COVID-19 pandemic and subsequently implemented in 2022, achieving 67.2% coverage (approximately 250,000 people treated) and meeting WHO criteria (“Pass”).
Following the second MDA, a Transmission Assessment Survey (TAS) was initially planned. However, implementation was postponed pending updates to WHO guidelines on post-IDA evaluation. After the revised guidance was issued in around November 2023, the first IIS was conducted between April and June 2024.
The survey was led by the ENBP Provincial Health Authority (PHA), with technical support from WHO and the project. Field implementation and monitoring were carried out by PHA staff, while laboratory analysis, including confirmation of microfilaria (Mf) *1, was conducted by the Papua New Guinea Institute of Medical Research (PNG-IMR) Kokopo team. The survey involved night blood collection in some areas and was implemented with strong community cooperation, taking into account safety and weather conditions.
As a result of the IIS implementation, of the 3,150 samples collected from 30 randomly selected survey sites across the state, 75 tested antigen-positive (antigen prevalence: 2.4%). Of these, only 2 samples from a single village among the 30 survey sites were confirmed to contain Mf (microfilariae), which is responsible for transmission of infection. This confirmed that the level of infection across the state is sufficiently low to be considered eliminable, and WHO assessed the province as “Pass,” indicating that additional province-wide MDA was not required. At the same time, taking into account the confirmed Mf-positive cases and the risk of further transmission, it was recommended that additional MDA be conducted on a targeted basis, limited to the affected areas.
| Year | Activities | JICA Project |
|---|---|---|
| 2019 | • Baseline survey conducted (Sep–Oct): antigen prevalence 5.0%, microfilaria (Mf) prevalence 1.2% • First round of MDA implemented (Nov–Dec): coverage 82.2% (Main partners: ENB Provincial Government, WHO, JICA, etc.) |
Technical Cooperation: Project for Elimination of Lymphatic Filariasis in the Pacific Region -Phase 1 (Oct 2018–Feb 2022; extended one year due to COVID-19, completed Feb 2023). |
| 2022 | • Second round of MDA implemented (Apr–Jun): coverage 67.2% (Main partners: ENB District Development Authorities(DDAs), WHO, JICA, etc.) |
|
| 2024 | • First IIS conducted (Apr–Jun): antigen prevalence 2.4%, Mf prevalence 0.06% • IIS result: WHO assessment “Pass” (no additional province-wide MDA required; targeted MDA recommended in areas with potential higher risk) (Main partners: JICA, ENBPHA, PNG-IMR, WHO, etc.) |
Technical Cooperation: Project for Elimination of Lymphatic Filariasis Phase 2 (Apr 2024-Apr 2027). |
Planning and Implementation of Focal MDA
In response, the PHA, with support from WHO and the project, coordinated the implementation of focal MDA in four areas identified through IIS findings and previous evidence. The activity was jointly financed by WHO, the project, and the PHA.
Preparations faced several challenges. In May 2025, a circulating vaccine-derived poliovirus (cVDPV2) outbreak was confirmed in Papua New Guinea, prompting a nationwide immunisation campaign targeting children*2. As this became a top priority, it affected the availability of personnel and delayed preparations for the focal MDA. In particular, PHA staff had to manage multiple responsibilities, including immunisation activities and monitoring and evaluation tasks, often under demanding field conditions.
Despite these constraints, the activity proceeded following extensive coordination among stakeholders. After the second round of the polio campaign was underway, a refresher training for 22 health workers was conducted in Kokopo on 14 November 2025. The focal MDA was then launched shortly thereafter and completed in early December. Final reporting, including financial verification, is currently being finalised by the PHA in coordination with the National Department of Health (NDoH) and WHO (As of May 2026, reporting and financial reconciliation are still ongoing).
The project supported the procurement of supplies, transportation of medicines and materials from Port Moresby, fuel procurement, and data management. The IDA medicines used in the campaign were donated by pharmaceutical companies through WHO’s donation programme and supplied to the Government of Papua New Guinea
*3
.
In this way, even within limited human and financial resources, the collaboration/partnership among relevant stakeholders enabled the implementation of additional MDA activities to prevent further transmission of LF, which can be regarded as an important achievement in ensuring the continuity of infectious disease control efforts in the province.
Location of East New Britain Province (highlighted in green) (MapChart)

Group photo from the refresher training for PHA staff (Kokopo PHA Headquarters)

Drop-off of boxes containing MDA supplies and medicines for Kokopo at an air freight company in Port Moresby.

Treatment recording register used during field activities. Previously managed using separate sheets, the format and printing process were improved to enhance efficiency.
Timeline
| July 2024 | Completion of the first IIS; feedback on the survey report received from WHO |
| March 2025 | Decision made to conduct targeted MDA in selected areas based on IIS results |
| August 2025 | Consultation with the PHA on the budget and implementation plan for the focal MDA (Kokopo) |
| September 2025 | Medicines and related supplies transported by air |
| November 2025 | ・Sorting and preparation of medicines and supplies ・Refresher training conducted for PHA personnel (Kokopo) ・Launch of focal MDA activities (approximately three weeks) |
| December 2025 | Completion of focal MDA activities |
Implementation and outcomes of focal MDA in hard-to-reach areas
This activity was implemented from mid-November to December 2025 across four target areas, reaching approximately 2,300 residents
*4
. While this represents a limited proportion of the provincial population (around 0.6%), the activity was strategically targeted at high-risk areas for transmission and is expected to contribute effectively to reducing further spread of infection.
The focal MDA targeted four areas: Karawara and Utuan in Kokopo District (Duke of York Islands)*5, and Manigugule and Buka in Pomio District. Karawara, Utuan and Buka were identified as high-risk areas for LF transmission based on a survey conducted by Case Western Reserve University around 2023*6, while Manigugule was an area where microfilariae (Mf) were detected in the earlier IIS. These areas include locations with difficult access, such as remote islands requiring sea transport and inland areas accessible only via unsealed roads, and a number of operational constraints were anticipated in implementing the activities.
Focal MDA activities commenced on 17 November 2025, starting sequentially in areas where preparations had been completed, and were implemented within the planned timeframe while maximising the use of limited resources. Field operations, as well as monitoring and supervision, were primarily led by PHA staff, with partial support from staff of the NDoH. Field teams visited target communities, including residents with prior MDA experience, and provided advance explanations (toksave) on the effectiveness and safety of the treatment, while encouraging community participation in LF elimination efforts. In some cases, teams travelled between villages with overnight stays, requiring intensive and well-coordinated implementation within a short period. In certain areas, particularly in Manigugule, temporary interruptions occurred due to prolonged adverse weather conditions, including river flooding and fallen trees, which made access difficult. However, activities resumed with due consideration for safety and improving weather conditions, and all planned activities across the target areas were successfully completed by around 6 December 2025.
Data management was facilitated through a WhatsApp-based reporting system established by the project, through which each team shared daily updates, enabling real-time monitoring and data consolidation. Final data records were handed over to the PHA, together with returned materials, for further management and consolidation. According to field reports, no serious adverse events related to treatment, nor any major incidents during implementation, were observed, and the activities were carried out safely through close coordination among stakeholders.
As a result, treatment coverage rates ranged from 81.3% to 110.8% across the target areas, achieving an overall coverage rate of 95.2%. In addition, a total of 24 suspected LF cases were identified during the activities, including 20 cases of limb lymphoedema, 3 cases of hydrocele, and 1 case of breast oedema. These cases will be followed up on and referred to appropriate medical care going forward.
Activity Overview
| 1.Target population | Approximately 2,300 people in the selected areas*7
(Based on population data maintained by the PHA) |
| 2.Target areas | Kokopo District 1. Karawara (Duke of York Rural LLG) 2. Utuan (Duke of York Rural LLG) Pomio District 3. Manigugule (Moke Moke) (Central-Inland Pomio Rural LLG) 4. Buka (Central-Inland Pomio Rural LLG) |
| 3. Period | November–December 2025 (Approximately 3–10 days per area) |
| 4. Approach | ・Treatment was administered using directly observed treatment (DOT) *8, through house-to-house visits, schools, workplaces, and community gatherings, depending on local conditions. Dosing was determined based on height and age, and treatment records were documented and compiled. ・Suspected LF cases identified during the activity were recorded and reported for follow-up. |
| 5.Structure | The activity was carried out by seven teams across the four target areas (two teams each in Karawara, Utuan, and Manigugule, and one team in Buka). Each team consisted of two health workers, two community volunteers, and one additional member (such as a boat operator or driver), with approximately five members per team. |
| 6. Budget | Total estimated cost: approximately PGK 67,000*9
(Approx. JPY 2.5 million / USD 18,000) (Major contributors: WHO, LF project (JICA), and PHA) |
| 7.Use of results | ・Results will be reported by the PHA to WHO and reviewed accordingly. ・The list of suspected LF cases will be used by the PHA to support continued care and case management. |
Location map
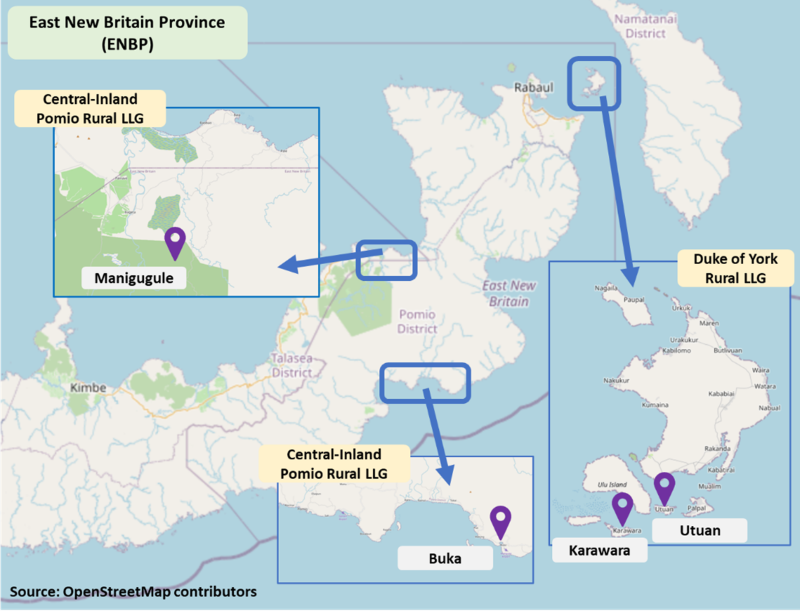
Table 1. Focal MDA results by area (based on PHA population data)
| District | Area | Target population | # of people administered (female/male) | Focal-MDA coverage (%) | # of IVM administered | # of D1EC administered | # of ALB administered |
|---|---|---|---|---|---|---|---|
| Kokopo | Karawara | 716 | 669 (358/311) | 93.44 | 2,571 | 2,595 | 669 |
| Kokopo | Utuan | 952 | 874 (520/354) | 91.81 | 3,422 | 3,451 | 874 |
| Pomio | Manigugule | 500 | 554 (262/ 292) | 110.80 | 1,702 | 1,746 | 554 |
| Pomio | Buka | 230 | 187 (107/80) | 81.30 | 616 | 620 | 187 |
| Total | Total | 2,398 | 2,284 (1,247/1,037) | 95.25 | 8,311 | 8,412 | 2,284 |
| *IVM: Ivermectin; DEC: Diethylcarbamazine; ALB: Albendazole | |||||||
Table 2. Profile of suspected lymphoedema cases
| Condition | Number of cases | Sex (F/M) | Mean age (years) (Total/F/M) | Mean duration of symptoms (years) (Total/F/M) | |||||
|---|---|---|---|---|---|---|---|---|---|
| F | M | Total | F | M | Total | F | M | ||
| Limb lymphoedema | 20 | 12 | 8 | 47.6±15.5 | 42.7±14.8 | 55.0±14.1 | 11.8±14.1 | 3.8±5.3 | 25.4±14.1 |
| Hydrocele* | 3 | 0 | 3 | 63.3±7.6 | - | 63.3±7.6 | 24.7±12.7 | - | 24.7±12.7 |
| Breast oedema | 1 | 1 | 0 | 35.0±0.0 | 35.0±0.0 | - | 13.0±0.0 | 13.0±0.0 | - |
| *Includes cases with concurrent limb lymphoedema | |||||||||

Practical training session conducted by refresher training participants for other health workers prior to the MDA (Open Bay Health Centre)

Reviewing MDA treatment records in the field (Karawara)

Distribution of medicines to community members following height measurement and registration (Utuan)

Administration of treatment using directly observed treatment (DOT) under supervision of health workers (Karawara)

Community awareness session on MDA and skin diseases conducted by the field team ahead of treatment activities (Manigugule)

Mop-up visit to previously covered areas to check for community members who may have missed treatment (Utuan)

Temporary repair of a damaged unsealed road following rain during the return way from field activities (Manigugule)

Field team crossing a makeshift bridge formed by a fallen tree while travelling to a remote community (Manigugule)

Mild suspected LF case identified during the activity (female, Utuan)

Severe suspected LF case with deep skin folds identified during the activity (male, Utuan)
Future actions towards advancing sustainable disease control
The additional MDA contributed to reducing residual transmission in high-risk areas and strengthened coordination among stakeholders, particularly through PHA-led implementation. It is also expected to help reduce infection risks among communities and encourage early care-seeking behaviour. This activity contributes to progress towards the WHO NTD Roadmap 2030*10 targets for the elimination of lymphatic filariasis.
Moving forward, preparations are underway for the second IIS, alongside efforts to strengthen ongoing monitoring and surveillance. Beyond the project period, it is expected that the Government of PNG will take the lead in continuing LF elimination efforts in collaboration with relevant partners.
Notes
*
1. Microfilariae (Mf) are the larval stage of the parasites that cause lymphatic filariasis and are commonly used as an indicator of infection.
*
2. On 9 May 2025, the Government of Papua New Guinea reported the detection of circulating vaccine-derived poliovirus type 2 (cVDPV2) in two children in Morobe Province to WHO. The country previously declared an outbreak of cVDPV1 in 2018.
Source: WHO, Circulating vaccine-derived poliovirus type 2 (cVDPV2) – Papua New Guinea
https://www.who.int/emergencies/disease-outbreak-news/item/2025-DON571
*
3. IDA medicines are provided free of charge to endemic countries through pharmaceutical donation programmes coordinated by WHO.
Source: WHO, Preventive Chemotherapy
https://www.who.int/teams/control-of-neglected-tropical-diseases/interventions/strategies/preventive-chemotherapy
*
4. According to the 2024 Population Census published in October 2025, the population of East New Britain Province is 367,093. The number of people treated through this focal MDA represents approximately 0.6% of the provincial population.
Source: National Statistical Office, 2024 Population in Papua New Guinea
https://www.nso.gov.pg/statistics/population/
*
5. The Duke of York Islands are located off the coast of Kokopo in East New Britain Province, Papua New Guinea, between New Britain and New Ireland, and consist of approximately ten islands.
Source: Wikipedia, Duke of York Islands, Papua New Guinea
https://en.wikipedia.org/wiki/Duke_of_York_Islands
*
6. A field study conducted in 2023 by Case Western Reserve University identified microfilaria (Mf) positivity in several areas, including Karawara and Utuan, suggesting a risk of residual transmission.
Source: Bun, K. et al., PLOS Neglected Tropical Diseases, 2025
https://pubmed.ncbi.nlm.nih.gov/39869653/
*
7. Under WHO guidelines, certain groups—including pregnant women, individuals with severe illness, and young children below a specified age—are excluded from MDA for safety reasons.
Source: WHO, Guideline: Alternative mass drug administration regimens to eliminate lymphatic filariasis, 2017
https://www.who.int/publications/i/item/9789241550161
*
8. Directly Observed Treatment (DOT) is a method in which trained personnel directly observe individuals taking medication to ensure proper administration. It is one of the approaches recommended by WHO for MDA implementation and is widely used in disease control programmes.
Source: WHO, Guideline: Alternative mass drug administration regimens to eliminate lymphatic filariasis, 2017
https://www.who.int/publications/i/item/9789241550161
*
9. The estimated budget breakdown includes approximately PGK 13,000 for procurement and transport of supplies, PGK 30,000 for implementation costs (including personnel, travel, vehicle and boat hire, and fuel), and PGK 24,000 for monitoring activities. Travel costs for the project team (JICA) and WHO were covered separately and are not included in the total.
*
10. In 2021, WHO published the NTD Roadmap 2021–2030 to reduce the burden of Neglected Tropical Diseases (NTDs) and accelerate progress towards their control and elimination by 2030, guiding countries to strengthen actions based on progress and remaining challenges.
Source: WHO, The Road to 2030, 2021
https://www.who.int/publications/i/item/WHO-UCN-NTD-SAI-2022.2
For more information
Related page (this website)
Media coverage