- Home
- Technical Cooperation Projects
- Index of Countries
- Africa
- Ghana
- Project for Improving Continuum of Care for Mothers and Children through the introduction of Combined MCH Record Book
- Project News
- Results of Baseline Survey and Situation Analysis for the intervention of the Project in Ashanti Region
Project News
2019-09-30
Results of Baseline Survey and Situation Analysis for the intervention of the Project in Ashanti Region
In 2019, the project is planning to start more intensive capacity building activities on MCH RB in 7 focus districts[1] of Ashanti region. In order to assess the effectiveness of the activities and to study the current situation regarding Maternal and Child Health and Nutrition (MCHN), the project conducted a baseline survey and situation analysis study prior to the intervention.
Objective of the study
The main objective of the baseline assessment and situational analysis study was to provide insights on gaps to help the strategic packaging of the project interventions and provide detailed information on the status of MCHN service provision and utilization before the start of the project intervention.
Specifically, the study sought to:
- assess the level of effective utilization of MCH RB by health workers and mothers (pregnant and lactating women) before the introduction of the project interventions,
- assess the experience regarding uptake of the MCHN services and utilization of MCH RB among health workers and mothers,
- assess dietary intake of pregnant and lactating women and the feeding of children.
- explore main barriers to achieve expected health and nutrition behaviour changes to make recommendations to feed into the strategies and activities.
Methodology
The survey was conducted in July and August 2019. A quantitative approach was employed for both the Baseline Assessment and Situational Analysis study. In addition, a qualitative approach, including Focus Group Discussions and In-Depth Interviews, was employed in the intervention districts to complement the Situational Analysis study. The total sample for the quantitative study was 600 mothers (pregnant women, mothers after delivery and mothers with 6 to 11-month babies) and 120 health workers selected from the 6 selected (3 intervention and 3 control) districts[2]. In addition, a total sample of 60 mothers and 30 mothers, all including pregnant women, mothers after delivery and mothers with 6 to 11-month babies, were selected from the 3 selected intervention districts for the Focus Group Discussion and In-Depth Interviews respectively.
This is facility-based survey. District and facilities were randomly selected, and incidental sampling was adopted for interviewee; interviewee were pregnant women and mothers who came to facilities for services. Also, health workers who are working at antenatal care (ANC), delivery, postnatal care (PNC) and child welfare clinic (CWC[3]) were interviewed.
Main results of the survey
Continuum of Care
Continuum of Care is still a big challenge. Less than 30% received first ANC before 12 weeks at intervention districts. Less than 15 % of mothers received three PNCs in scheduled timing at both intervention and control districts. 59% of mothers with 6-11months' baby at intervention districts and 34% of those at control districts received CWC in scheduled timing.
Utilization of MCHRB
Recording of the MCH RB in both intervention and control districts is generally low; especially records on Body Mass Index, estimated desired weight range at Expected Date of Delivery, plotting on the growth chart, nutrition tables, developmental milestones checked (less than 20 %).
Diet and feeding
Exclusive breastfeeding practice is 43-53%. Meeting the consumption of animal source foods is 44-56% among pregnant women. More than 75% of pregnant women are meeting the Minimum Dietary Diversity (MDD, 5+ Food Groups) and Minimum Meal Frequency (MMF, 3+). More than 70 % of children are meeting the MDD (4+ Food Groups) and MMF (3+), and consuming animal source food.
Experience and satisfaction of pregnant women/mothers
Participants in the study had mixed experiences with health workers attitude; whereas some participants reported poor reception, disrespect, impatience, harsh treatments and lack of attention to delivering service to mothers as a common issue with health workers, other mothers interviewed reported being treated with respect, great attention, good communication among others. Self-introduction from health workers to mothers during the first visit are less than 30% at intervention districts. 48 - 71% of mothers were given the opportunity to ask any questions during the visits. 71-91% of mothers felt they were adequately informed about care and examinations. One of the mothers said, "They are free with us and it allows us to tell them our problems, they teach us how to feed our children and what we should give to them and they don't shout on us. That is the reason why I like them". The other said, "Some of the nurses don't also pay attention to us. They can tell us to put the baby on the scale and instead of them to read it, they will be doing something else."
Experience and knowledge of health Workers
More than 80% of health workers are very or somewhat satisfied with the MCHN services they are providing. More than half of health workers cannot tell the 3A steps of nutrition counselling (assessment, analysis and action) and the rights of patients stated in Ghana Patient Charter.
Child nutrition and barriers
More doer mothers than non-doer mothers know that feeding a baby with at least four of the different food groups daily leads to the baby getting sufficient nutrition for brain development and stronger immunity development. More doer mothers than non-doer mothers noted that supports from family members, caregivers and/or health care giver make it possible for them to feed their babies at least 3 meals daily. More doer mothers than non-doer mothers noted that support and education provided by health workers and their family/relatives' understandings make it easier or possible for them to exclusively breastfeeding babies for 6 months. One mother said, "Sometimes you the mother wants to follow exclusive breastfeeding, but the family members will be complaining saying all sorts of things. Sometimes when I am not there then my sister, for example, will give the child water when the child cries, so although I'm willing to follow exclusive breastfeeding my house people makes it difficult".
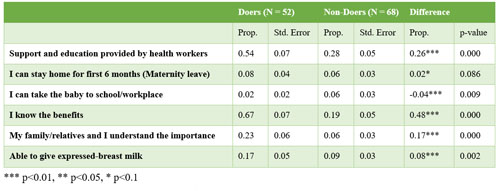 Table 1: Factors that makes it easier/possible for mothers to exclusively breast feed babies for 6 months
Table 1: Factors that makes it easier/possible for mothers to exclusively breast feed babies for 6 months
Mother nutrition and barriers
More doer mothers than non-doer mothers know that their fetus get all the necessary food and stronger immunity if they eat at least 5 of the different food groups daily. More doer mothers than non-doer mothers noted that they feel strong and healthy and develop strong immunity when they feed with at least one animal protein source daily.
Way forward
The project is going to start a series of health worker training in the focus districts, which will be followed by continuous monitoring and supervision. Behavior Change Communication activities will also be implemented to promote the effective use of MCH RB and healthier life of mothers and children. The end-line survey is going to be conducted in December 2020 to assess the effectiveness of the interventions.
Notes
- [1] The focus districts are Atwima Mponua, Atwima Nwabiagya, Amansie West, Amansie Central, Adansi North, Adansi South and Atwima Kwanwoma.
- [2] The intervention districts are Atwima Nwabiagya, Amansie Central and Adansi North. The control districts are Ejisu, Kwabre East and Asante Akim South.
- [3] Child Welfare Clinic is a service that allows parents to have babies and children under 5 years get weighed, length measured and immunized. Health/nutrition counseling is also provided.
- About JICA
- News & Features
- Countries & Regions
- Our Work
- Thematic Issues
- Types of Assistance
- Partnerships with Other Development Partners
- Climate Change / Environmental and Social Considerations
- Evaluations
- Compliance and Anti-corruption
- Science and Technology Cooperation on Global Issues
- Research
- JICA Development Studies Program / JICA Chair
- Support for the Acceptance of Foreign HRs / Multicultural and Inclusive Community
- Publications
- Investor Relations