Over one year has passed since the escalation in the intense conflict between Hamas and Israel. As the fighting has shown no signs of abating, JICA continues its humanitarian support in Gaza, utilizing the expertise developed within the Japan Disaster Relief (JDR) Team in collaboration with the WHO. Three team members are interviewed for their support from Japan.
Like a “living hell”: The unimaginable humanitarian crisis in Gaza
On October 7, 2023, Hamas, the militant group that controls the Gaza Strip in the Palestinian territories, launched a large-scale attack on Israel, and Israel retaliated with intense airstrikes. Now, over a year later, there is still no end in sight to the conflict, complicated by complex historical and geopolitical factors.
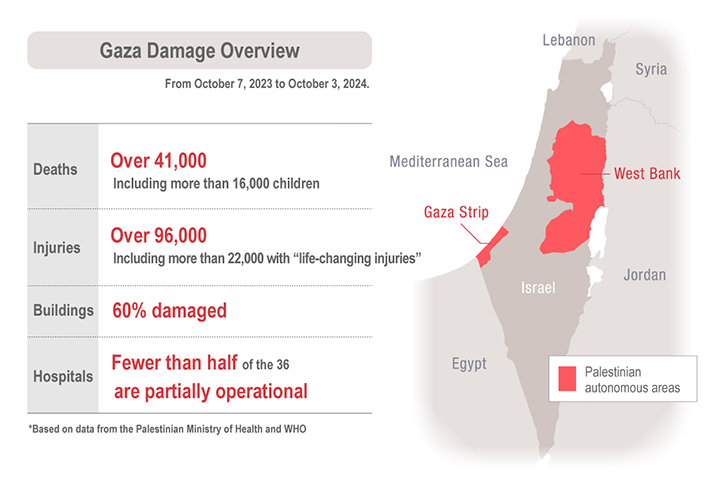
According to the Ministry of Health in Gaza, over 41,000 Palestinians have been killed and more than 95,000 injured in this conflict. About 60 percent of buildings in Gaza have been damaged, and more than half of the hospitals are no longer functional. Checkpoints have been closed, so humanitarian aid—including food, water, fuel, and medical supplies—is not reaching residents in sufficient amounts. Many Gazans are suffering from hunger and infectious diseases. United Nations Secretary-General António Guterres has warned that Gaza’s residents are “living in hell.”
The WHO requested JDR to provide support through MDS
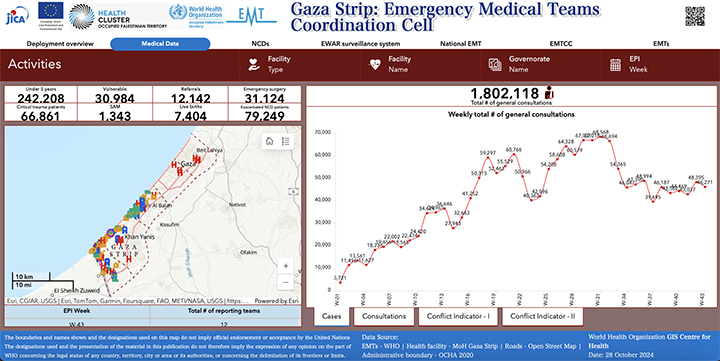
Around 17 Emergency Medical Teams (EMTs) are working tirelessly to provide care in Gaza. At first, the harsh conditions, such as a lack of internet and food, made it impossible to share information. No one, including the World Health Organization (WHO), had an accurate grasp of patient distribution, conditions, or medical needs. On October 13, the WHO requested the Japan Disaster Relief (JDR) Team to offer its expertise in data management.
The JDR Medical Team was deployed to provide medical support to the victims of the 2013 Philippines typhoon disaster. From that experience, the team developed an efficient method collecting essential data on the number and condition of patients treated by EMTs during disasters. The method, originally known as “SPEED” in the country, standardizes medical records and daily reports, facilitating easy and efficient data aggregation. It also visualizes the EMT activities in disaster areas, providing non-expert officials with vital information to better understand the situation and make informed decisions.
Later, this method was introduced to the disaster response scene in Japan as “J-SPEED” and formally adopted by the WHO as an international standard called the EMT Minimum Data Set (MDS). It has since earned global trust after being used in crises such as the March 2019 Mozambique cyclone, the February 2023 earthquake in Turkey, the 2023 flood in Libya, and in countries affected by the Ukraine conflict. The JDR Medical Team’s experience and expertise in data management, as well as the trust they have built with the WHO, led to the request for their support in Gaza.
Japan Disaster Relief (JDR)
The JDR is a Japanese relief unit dispatched upon request from the affected country’s government or international organizations to support overseas disaster relief efforts. It is comprised of five teams—the Medical Team, Rescue Team, Infectious Disease Response Team, Expert Team, and Self Defense Force Unit—with JICA serving as secretariat. At present, the JDR has been dispatched 168 times, including for the 2013 Philippines typhoon, the 2015 Nepal earthquake, and the 2023 Turkey earthquake. The JDR Law stipulates that it can only be deployed for natural disasters, which means humanitarian crises arising from conflict issues remain out of its scope. Nevertheless, JICA provides as much support as possible for humanitarian crises through other means, such as technical and financial cooperation. The Gaza mission marks the second case where the JDR’s expertise has been used for non-natural disasters, following support for Moldova, which had been affected by the Ukraine conflict.
-
*The JDR had been deployed for conflict-related emergencies until the enactment of the International Peace Cooperation Law in 1992.
Coordinated remote support from JDR members across Japan
Normally, support provided by JDR teams is conducted on-site, but due to restrictions on the movement of people and goods in and out of Gaza, as well as security concerns, it was extremely difficult for JICA personnel to enter the city. As a result, there was no choice but to provide support remotely this time.
Dr. Kai Soichiro from the Hyogo Emergency Medical Center has been involved in the Gaza support project since its early stages and has coordinated with the WHO. “When we first started remote support, we had to set up the foundation, such as a system for on-site EMTs to report their data,” he says.
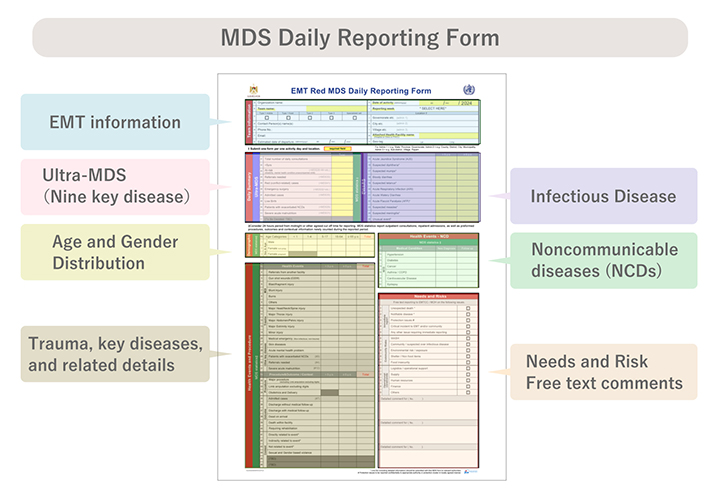
Kai explains how, in order to grasp the overall medical situation in Gaza, it is essential to collect daily data from the EMTs based on 50 MDS items, including patient age, gender, location, injury severity and type, as well as the presence of infectious diseases or pregnancies. “At the beginning, the framework for such reporting was not yet in place,” he says.
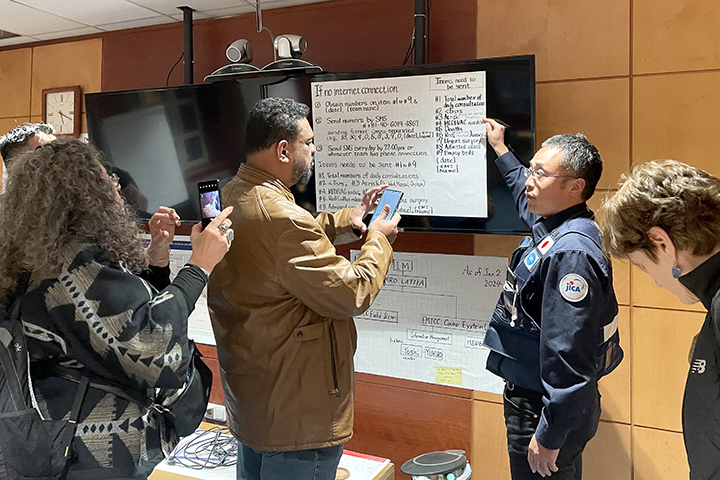
Normally, EMT Coordination Cells (EMTCC) set up by the affected country would consolidate data from EMTs. The situation, however, was different in Gaza. The region has strict entry restrictions, and with unreliable internet access, communication was severely hindered. From December to January, a total of eight members of the JDR Medical Team had to travel in shifts to Cairo, where they held direct discussions with the WHO and various EMTs entering and leaving Gaza. This emphasized the importance of reporting. They coordinated the necessary data items and laid the groundwork for remote support. Because of the harsh conditions, they began reporting on a reduced set of nine essential items from the original 50, known as the Ultra MDS, and gradually increased the number of items to include data on injuries and infectious diseases.
Ogawa Hanako is a nurse with nearly 20 years of experience, currently studying public health at Hiroshima University’s master’s program. She is leading the Data Entry Unit that corrects and inputs the MDS field reports into the required format. “Although we are not providing medical care directly to victims this time, I feel a great responsibility in relaying the reports to the WHO from the EMTs who are risking their lives,” she says.
The MDS reports sent from the field often have issues such as missing items, not following the required format, or are in handwritten form, making them difficult to compile. The Data Entry Unit of the JDR Medical Team re-enters the data according to the data sheet format. There is also a Double Check Unit that verifies the entered data, a System Management Unit that develops and operates data collection programs and ensures consistency, and a Communication Unit that coordinates with the WHO and other organizations. Up to 19 JDR members across Japan are divided into these units, working day and night to support the effort.
Tanaka Hideshige, president of an IT consulting company, is actively involved as the leader of the System Management Unit. “As a non-medical professional, my contributions are limited, but if there is something I can do, I want to support,” he says. “If there is work related to IT or data processing, I see it as my duty and mission to take on that role.”
All JDR members provide their services alongside their regular jobs or studies. Due to the seven-hour time difference with Gaza, data is submitted daily with a deadline of 9 p.m. JST, requiring late-night work. Thanks to their collaboration, the team members have maintained continuous support since the start. The data they collect is included in the WHO’s weekly situation report, released every Monday, which outlines the medical situation in Gaza.
Shared feelings and hopes regarding Gaza support
Tanaka has been concerned about the high proportion of child casualties since the beginning. As of July 2024, some 20 percent of injured and ill people are under 5 years old. “Not all the medical data is directly linked to the conflict, but seeing the deep suffering of the children reflected in the data is the hardest part for me,” he says.
Nurse Ogawa of the Data Entry Unit says the details in the reports are disquieting. “The free-text section of the reports we receive from the EMTs often contains details of the harsh conditions in conflict zones,” she says. “They report events such as ‘there was a bombing yesterday, and many injured were brought in,’ or ‘we are struggling to provide daily medical care due to a lack of supplies.’ Some teams also report their safety every day. The reality that people are working under such severe conditions weighs heavily on me.”
Dr. Kai, who helped set up the reporting system, says that it’s not unusual for the number of fatalities in the daily reports to exceed double digits. “In Japan, such numbers would only be seen in large-scale traffic accidents,” he says. “We can only provide support through data management, but we hope that our work will reduce the burden on the EMTs on the ground and allow them to find time for rest and sleep. Ultimately, we hope this will benefit the people of Gaza.”
The emergency response phase for natural disasters is said to be few months, but support for conflict is required as long as the conflict continues. The members share their hope that the conflict ends as soon as possible, and that they can shift to supporting the recovery and reconstruction. It is shared by all the international emergency relief personnel as they continue to support the medical efforts in Gaza.